


Embryo Transfer 101: Your Guide to Embryo Transfer During IVF


Medically reviewed by Linda Streety, RN, BSN
What is an embryo transfer?
Very simply, embryo transfer is a procedure in which your reproductive endocrinologist (RE) places an embryo (an egg that has been fertilized by a sperm cell) into your uterus. This is the final step of the in vitro fertilization (IVF) process!
Six Second Snapshot
- Embryo transfer is a simple, outpatient procedure that can be performed at your fertility clinic.
- Your clinician will use ultrasounds to guide a catheter loaded with your embryo(s) through your cervix and into the center of your uterus. Then your clinician will release the embryo-containing fluid into your uterus.
- A fresh embryo transfer usually occurs 3-5 days after egg retrieval. If you decide to freeze (cryopreserve) any of the eggs or embryos, you can transfer an embryo weeks, months, or even years later!
When does embryo transfer occur?
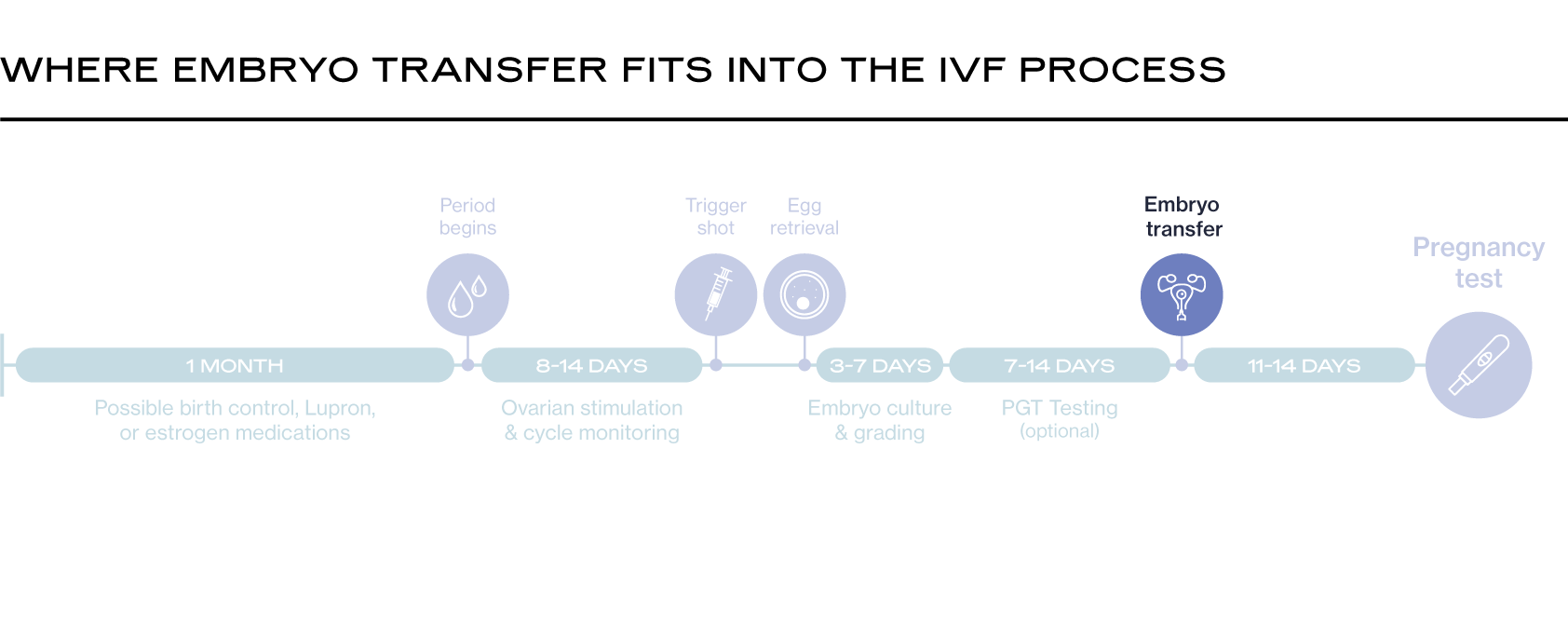
Embryo transfer happens after all the other steps of your IVF cycle:
- Ovarian Stimulation: hormone medications stimulate the ovaries to produce multiple egg containing follicles.
- Egg Retrieval and Sperm Collection: Eggs are removed from the ovaries in a simple surgical procedure. Sperm collection can be very simple, but in the case of severe male factor infertility, it may involve a procedure to remove sperm directly from the testicles.
- Fertilization and Embryo Growth: The eggs are fertilized in a lab with the sperm, and incubated for 3-7 days. An embryologist “grades” any embryos that result from this process to determine which ones have the strongest chance of success.
- Embryo Transfer: An embryo (usually just one) is transferred to the uterus in a simple outpatient procedure.
A fresh embryo transfer usually occurs 3-5 days after egg retrieval in your IVF timeline. If you decide to freeze (cryopreserve) any of the eggs or embryos, you can transfer an embryo weeks, months, or even years later!
What happens during embryo transfer?
Embryo transfer is a simple, outpatient procedure that can be performed at your fertility clinic. It does not require sedation or anesthesia, though your clinician may prescribe a muscle relaxant. If your clinic permits it and you have a partner, your partner can join you for the procedure.
You will likely be asked to arrive with a comfortably full bladder. This is because the procedure uses an external (abdominal) ultrasound to place the embryo in just the right spot. A full bladder helps your clinician view your uterus.
When you are ready for the transfer procedure, your embryo or embryos will be loaded into a long, slim catheter with some fluid. A speculum will be inserted into your vagina, and your clinician will use both external and internal ultrasounds to guide the catheter through your cervix (you will likely feel some discomfort, similar to a pap smear) and into the center of your uterus. They will be taking care to ensure that the catheter is in just the right spot. Then your clinician will release the embryo-containing fluid into your uterus. After removing the catheter, your clinician will check to make sure the embryo is not still inside the catheter. (If it is, they will repeat the procedure right then!)
You will have some time to rest at your clinic before going home.
A day or two after embryo transfer, your embryo will hopefully hatch out of its shell and implant in your uterine lining (also known as the endometrium). However, it will take some time for levels of human chorionic gonadotropin (hCG), the hormone produced by the placenta, to rise enough in your blood to be detected on a beta hCG blood test, which your clinician will use to confirm your pregnancy.
What are the different types of embryo transfer?
Fresh Embryo Transfer
A fresh embryo transfer occurs 3-5 days after egg retrieval. The advantages of a fresh transfer are that it shortens the time you must wait to get pregnant, and it reduces the risk of losing an embryo during cryopreservation.
However, cryopreservation techniques have improved so much in recent years that frozen embryo transfers are just as successful – and sometimes more so – than fresh transfers. Additionally, it can be hard for your body to go from the elevated hormones of egg retrieval straight into a pregnancy, since the hormones used to control ovulation can interfere with uterine lining receptivity (how well the embryo can attach to your uterus).
Fresh transfer may not be the right choice for you if you have elevated progesterone levels after egg retrieval, or if you are at risk of ovarian hyperstimulation syndrome (OHSS) which can worsen after embryo transfer.
A fresh embryo transfer can occur on either day 3 or day 5 of embryo development:
- Day 3 Fresh Embryo Transfer: At day 3, embryos are at the “cleavage” stage of development, and contain about 6-8 cells. Clinicians sometimes choose to transfer embryos at this stage since the uterine lining is the optimal place for embryos to grow, rather than in a lab. The thinking is that an embryo that may not make it to the blastocyst stage in a lab may thrive in the uterus. Because it’s hard to tell at this stage how healthy the embryos are, transferring multiple embryos is more common during a Day 3 transfer, and carries a higher risk of having a multiple pregnancy. A Day 3 embryo transfer may also be the more financially conservative option because it reduces the cost of lab culture and eliminates the cost of cryopreservation.
- Day 5 Fresh Embryo Transfer: By day 5, embryos often have reached the “blastocyst” stage and have divided into two types of cells: the cells that will become the fetus and the cells that will form the placenta. Embryos transferred at this stage are placed in the uterus at the same time in your cycle as an embryo would if it traveled naturally down your fallopian tube, so the timing means that your uterine lining is optimized to receive the embryo. The reasoning in doing a Day 5 embryo transfer is that it’s easier to assess whether an embryo is of a high quality at this stage, and therefore likely to progress into a pregnancy. Transferring on Day 5 is increasingly common as lab culture systems have improved, and usually is conducted as a single embryo transfer.
Frozen Embryo Transfer
If you opt for frozen embryo transfer (FET), your clinician will likely have you wait at least one full menstrual cycle - about 6-8 weeks – before your transfer. This allows your body to recover from the egg retrieval process so your uterine lining is primed for pregnancy. You can also wait much longer before embryo transfer! IVF success rates are determined by the age of the person providing the eggs at the time of egg retrieval; your age at embryo transfer is less important to your chance of success.
If you are concerned about genetic or chromosomal abnormalities which can increase your chance of miscarriage or cause lifelong disability for your child, you may opt to do preimplantation genetic testing (PGT) on your embryos. If you decide to do PGT, you will have a frozen embryo transfer.
As part of the frozen embryo transfer process, you may need to supplement with progesterone to help your body support your pregnancy in its earliest stages.
- Natural Frozen Transfer: During a natural frozen transfer, your clinician will time your embryo transfer to coordinate with when you naturally ovulate. This is because your uterine lining will be primed to accept an embryo at this point in your menstrual cycle. If you are producing progesterone on your own, you can opt for a natural frozen transfer. Your clinician may supplement this process with hormones. While the timing still coordinates with your natural cycle, an hCG shot can ensure that you ovulate, and supplemental progesterone can ensure that your body can support an early pregnancy.
- Medicated Frozen Transfer: In this type of frozen transfer, your clinician will prescribe estrogen and progesterone medications (and sometimes gonadotropin-releasing hormone, or GnRH) to optimize your uterine lining for pregnancy. This is important if your body is not producing progesterone on its own. You may begin medication before embryo transfer and continue for weeks afterward. As far as embryo transfer success rates go, a retrospective study published in Fertility and Sterility of 1,455 fresh transfer cycles and 1,455 frozen-only transfer cycles found that while the pregnancy rates were about the same for patients under 35, freeze-only cycles were more likely to result in pregnancy for patients over 35 (1).
How can I best prepare for embryo transfer and what steps can I take to ensure success?
If your clinician has prescribed fertility medications for you to administer before and throughout the embryo transfer process make sure that you take them every day! Consistency with hormone medications is important to the success of the IVF process.
You can also take steps to optimize your uterine lining, such as ensuring that you are getting enough Vitamin E, taking L-Arginine supplements, and even getting acupuncture, which has been shown to have a positive effect on endometrial receptivity!
You may be worried that resuming regular exercise may harm your chance of success. However, a study published in Reproductive Biomedicine Online of fifty women undergoing embryo transfer found no difference in success rates between patients who resumed regular activity immediately and ones who lessened activity. The study concluded that patients could resume regular physical activity immediately after embryo transfer without adverse effect (2).
Recent Articles
References

-
Wang, Ange, et al. “Freeze-Only versus Fresh Embryo Transfer in a Multicenter Matched Cohort Study: Contribution of Progesterone and Maternal Age to Success Rates.” Fertility and Sterility, vol. 108, no. 2, 1 Aug. 2017, pp. 254-261.e4, www.fertstert.org/article/S0015-0282(17)30363-1/fulltext, https://doi.org/10.1016/j.fertnstert.2017.05.007.
-
Zemet, Roni, et al. “The Association between Level of Physical Activity and Pregnancy Rate after Embryo Transfer: A Prospective Study.” Reproductive Biomedicine Online, vol. 42, no. 5, 1 May 2021, pp. 930–937, https://doi.org/10.1016/j.rbmo.2021.01.013. Accessed 1 June 2023.
Share this
Recent Articles


Learn everything you need to know about IVF
Join the newsletter for IVF education, updates on new research, and early access to Alife products.






Sign up for our newsletter for the latest advancements in fertility care.
©2026 by Alife Health
Terms
Privacy
App Privacy
Security
Cookie Declaration
[website version: 740-00200-REC-01 Rev 2]



